"*" indicates required fields
General And Emergency Dental Treatment
Connor Referral
Question? Ask us here!
Please ask any specific question you have here, and one of our friendly dental team will shortly respond to you with an answer.
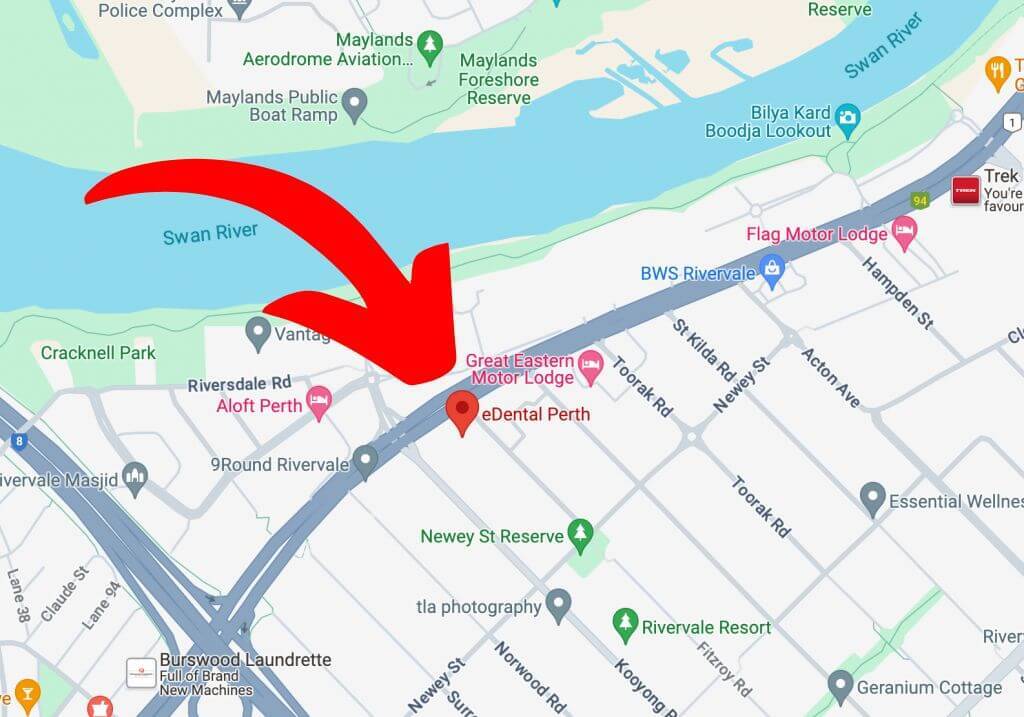
Eastgate Commercial Centre
14/49 Great Eastern Hwy
Rivervale WA 6103
Open 7 days, 8am - 8pm*
1300 467 112
* Appointments after 5pm on Sunday may require a prior booked appointment.